 A 32-year-old newly transferred inmate tells the medication nurse he sees blood in his urine. The nurse asked him to submit a sick call slip. Ten days later he is taken to the emergency room with flank pain and hematuria, having not yet been seen in sick call. A review of his chart indicated he was on a standing dose of 5mg of Coumadin (warfarin) without any INR orders since before the transfer from a facility two hours away.
A 32-year-old newly transferred inmate tells the medication nurse he sees blood in his urine. The nurse asked him to submit a sick call slip. Ten days later he is taken to the emergency room with flank pain and hematuria, having not yet been seen in sick call. A review of his chart indicated he was on a standing dose of 5mg of Coumadin (warfarin) without any INR orders since before the transfer from a facility two hours away.
Unfortunately, this is a snippet from an actual situation. It underscores the often disconnected nature of correctional health care and the need to have a well-established system to monitor the effects of high-risk medications like Coumadin (warfarin). The medication nurse had not made the connection between the patient’s bleeding and the medications she was administering. It is apparent that there are several patient safety issues here. What questions do you have about this case? Here are mine.
- Why did the nurse not connect bleeding with the patient’s medication profile?
- Did the patient follow through with submitting a sick call slip?
- How was the sick call request triaged? Why was bleeding not prioritized to be immediately scheduled for an evaluation?
- Why is Coumadin given without an INR order?
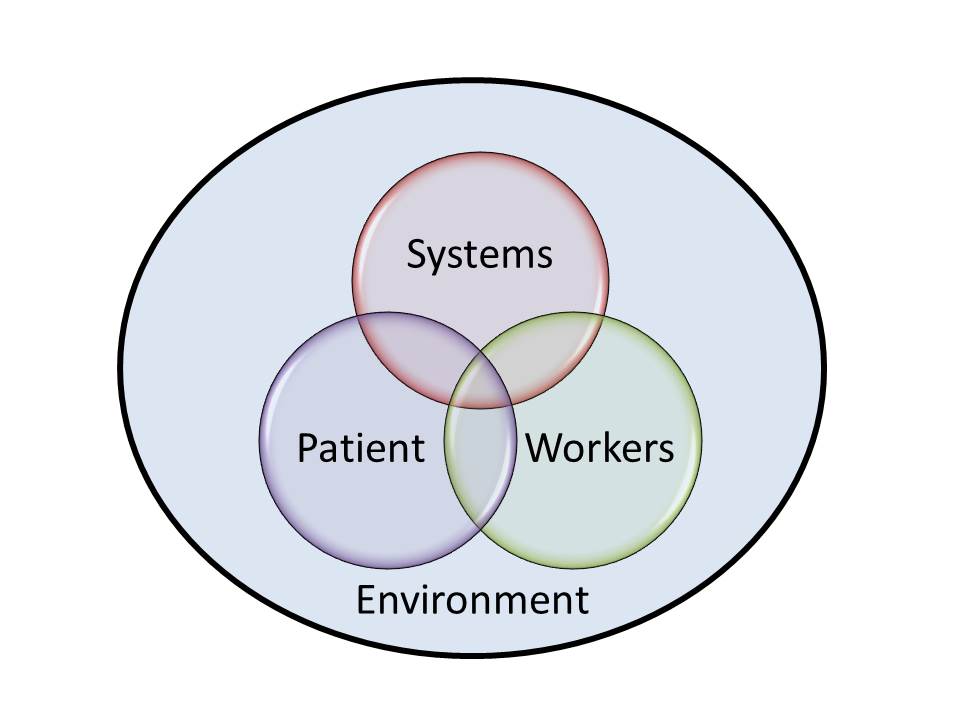
When I evaluate a patient safety issue such as this one, I use a 4-part model that takes into account the components of care environment, therapeutic systems, patient involvement, and care givers in determining how to make improvements and learn from the experience. This model is described in detail in my book “The Correctional Health Care Patient Safety Handbook” and assures a thorough evaluation of all possible elements. Let’s take a look at the situation from this four-fold model.
Environment
The environment of care is both the physical environment and the organizational culture of the workplace. As you might imagine, this component is the most difficult to change in any setting. Correctional facilities are set up for security and not for health care delivery. Medication administration often takes place in the housing area or a location away from the medical unit such as the dining hall or rec yard. The patient’s medical information, other than the MAR, is often unavailable.
The organizational culture is also based on security need rather than health care consideration. Many a nurse is pressured to administer medication in an unreasonably short time period based on inmate movement and the security schedule. It is easy to develop tunnel-vision when 200 inmates are on the docket for morning meds.
Systems
Standard systems for high-risk processes can reduce the chance of situations like the one described here. The therapeutic response to medications is often monitored during chronic care visits and this patient should have been on the roster for regular attention to his blood disorder. However, therapeutic blood levels should have been a standard part of every Coumadin (warfarin) medication order to decrease the chance of situations like this. In fact, the following medications should be titrated based on blood levels:
- Anticoagulants (warfarin/heparin)
- Digoxin
- Dilantin
- Lithium
- Theophylline
Patient
In this case, the patient could have been a help in monitoring the medication effect. He was knowledgeable about his condition and initiated communication with health care staff about his concerns. Patients can be very helpful in reducing medication errors and improving monitoring efforts. See this prior post about ways your patient can help you avoid medication errors.
Care Givers
The staff member delivering medication at the point of care is the last barrier against error. In a chaotic work environment where health care tasks may be disjoint and fragmented, staff members can easily develop a task-based model of care. There are indications of this mindset in this case as the nurse directs the patient to go to sick call rather than hearing the concern from the contact of the total patient situation. In addition, bleeding is a high-level concern, no matter the reason, and this patient needed immediate, rather than delayed attention. Other caregiver concerns to explore include a lack of knowledge, cynicism, and fatigue.
Monitoring the effects of medication is a correctional nurse challenge. How do you deal with this in your setting? Share your tips in the comments section of this post.
Check out Correctional Health Care Patient Safety Handbook for more information about this topic. Click this image below:
Gayle Burrow says
A very good article, Lorry. The first lesson is the have a skilled nurse in booking/receiving to obtain as comprehensive history and assessment as possible. Then follow up with the information and document. The patient may have been so busy worrying about going to court and his family, he did not submit a request for care. However, the nurse in booking should have initiated a plan of care with a checks by nurses, a urine specimen and a call to the provider for initial orders with bleeding. The nurse who was giving the medications, let the patient down by not realizing the seriousness of Coumadin. We all can learn from this story.