Osteoarthritis and Rheumatoid Arthritis are both debilitating diseases that affect millions of individuals in the United States. In the correctional environment, the latest statistics by the Bureau of Justice indicate that “Arthritis” is the third largest chronic diagnosis for jail detainees and is the second largest chronic diagnosis for individuals incarcerated in prisons. Osteoarthritis and Rheumatoid Arthritis are often thought of as the same, but they are different diseases with different etiologies and somewhat different treatments.
Today we will be discussing Rheumatoid Arthritis. Rheumatoid Arthritis is a chronic, progressive, and erosive disease characterized by recurrent inflammation of the connective tissue, primarily in the joints. Rheumatoid arthritis can also affect the organs of the body, such as the heart, lungs, and the endothelial cells of the vascular system. A cardinal sign of Rheumatoid Arthritis is the symmetry of the effect on the body; that is, it most often affects the left and the right sides the same.
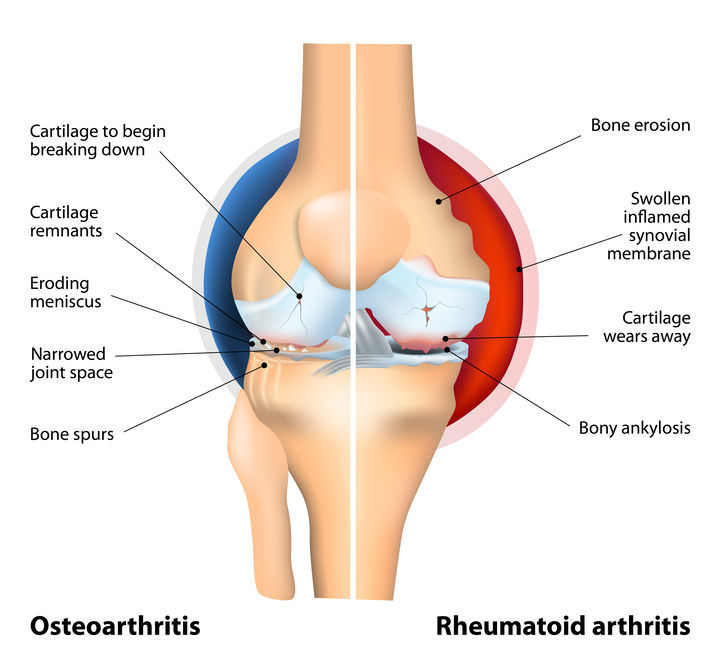
Rheumatoid arthritis
Rheumatoid arthritis (RA) is a chronic, progressive and erosive disease characterized by recurrent inflammation of the connective tissue, primarily in the joints. There are also a range of systemic effects that occur. RA affects approximately 2% of all adults, and in the United States, approximately 1.5 million people have RA.
RA most often begins with inflammation of the synovial membrane, which becomes thickened and swollen, and causes erosion of the articular cartilage and underlying bone. This then causes the joint to erode. RA typically affects the joints symmetrically; that is, what occurs on the left side of the body most often also occurs on the right. The small peripheral joints of the hand and wrist and the joints of the knees, ankles, elbows, and shoulders are usually affected first, but the cervical spine may also be affected. Extra-articular involvement of the disease includes inflammation of the tendon sheaths; the bursae; and the connective tissue of the heart, lungs, pleura, and arteries. Patients with RA commonly have nodules and deformity, most often of the metacarpophalangeal and proximal interphalangeal joints. One such deformity, the hyperextension of the proximal interphalangeal joints is also known as “swan neck” joints.
Common symptoms include morning joint stiffness, symmetrical joint pain and tenderness in the small joints of the hands and feet, and joint swelling. Many patients experience systemic effects such as fever, weakness, fatigue, and malaise before joint swelling actually occurs. As the disease progresses, patients may experience deformity, limited range of motion, and rheumatoid nodules. The most common joints involved are the metacarpophalangeal (MCP- knuckles of the hand) joints, the wrist, the proximal interphalangeal joints, the knee, the metatarsophalangeal (MTP-feet) joints, the shoulder, and the ankle.
The complications of RA include temporomandibular joint disease, infection, osteoporosis, myositis, cardiopulmonary lesions, lymphadenopathy, and peripheral neuritis. Although the specific cause of RA unknown, current theories include infection, autoimmunity, genetic factors, and environmental and hormonal factors. Heredity seems to account for 50% of the risk for RA, with other risk factors to include imbalance of intestinal microbes, cigarette smoking and nicotine exposure, diet with high sugar content, obesity, hormone imbalances, infection with Epstein-Barr virus, and environmental exposure.
NURSING INTERVENTIONS FOR THE PATIENT WITH Rheumatoid ARTHRITIS
Patient Education
The goals of treatment for RA are to relieve pain, inhibit the inflammatory response, preserve joint function, and prevent deformity. Initial medical treatment most often consists of pharmacologic measures.
An appropriate ongoing exercise program should be encouraged; and the teaching of proper body mechanics is an important aspect of every exercise program. If necessary, the patient can apply moist heat with facecloths/towels to relieve joint pain and to help with range of motion exercises.
During acute stages of the disease, the patient should be encouraged to avoid exercising the inflamed joints, while understanding that he/she needs to maintain mobility and movement of joints that are not involved. Thus, the need for rest of the affected joints should be part of the patient education during the acute phase.
Splints may be prescribed for painful joints and in the correctional environment, some creativity might be necessary to get the desired effect within security regulations.
Medication
The patients prescribed calcium metabolism modifiers, NSAIDs, and salicylates may need periodic laboratory monitoring of liver and kidney functioning. While the ordering of such testing is the responsibility of the provider, the nurse should expect to obtain the specimens.
Patients should be taught common drug interactions for the medications they are prescribed. They should be instructed not to take over-the-counter drugs or change the dosage of prescribed NSAID medications without consulting the healthcare staff. Instructions regarding medication should include the importance of taking medications with food or right after meals to minimize the potential for gastrointestinal discomfort.
Methotrexate should never be taken before confirming that the female patient is not pregnant.
Finally, as with all nursing encounters, be sure to document all in the health record, including patient teaching given, the patient’s comprehension, and the patient’s response to any nursing intervention provided.
Information for this blogpost is taken from The Correctional Nurse Educator class entitled Arthritis for the Correctional Nurse.
Please share your experiences caring for arthritis patients in the comments section below.