A 33 year old male patient from a maximum security state prison was admitted to a community hospital with flank pain and hematuria. His INR was discovered to be 8.2 (therapeutic range 2-3). His medical history included deep vein thrombus resulting from Protein S deficiency. A medication error investigation revealed that the patient had been receiving three times the amount of the current order of warfarin (Coumadin) and no INR diagnostic tests had been completed for the last 2 weeks.
Investigating What Went Wrong
Hundreds of doses of medication are administered every day in most correctional facilities, so it is not surprising that errors involving medication administration and management are plentiful. Investigating errors can reveal important information necessary to make improvements and reduce future risk. An error can occur from poor decisions and actions along the entire medication management system: ordering, transcribing, dispensing, administering and monitoring. Often an incident review reveals poor practices in several areas that contributed to the error.
Blunt End/Sharp End Evaluation of Clinical Errors
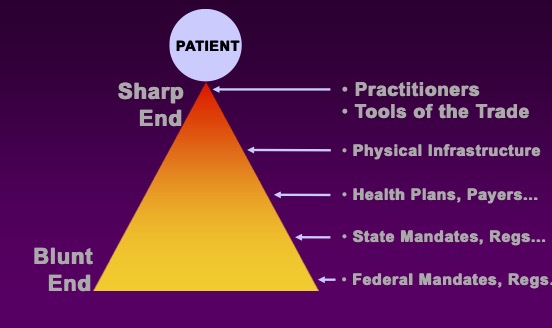
A helpful model of error causation, Blunt end-Sharp end, looks at the various components of a clinical error as an inverted triangle with the point of care being at the sharp end and the various complexities of organizational structure, system, policies and processes being at the blunt end, and removed from the actual error episode. Blunt end components, then, contribute to an environment that either encourages or does not prevent the error under consideration.
Case Analysis by Blunt End/Sharp End
The Blunt End/Sharp End model provides a framework for evaluating a clinical error like the one described above.
Sharp End: Investigating the sharp end of the error focuses on the actions of the clinicians in direct contact with the patient. Here are some sharp end investigation questions for this case:
- Did the nurse follow standard medication administration safety steps when administering the recent doses of warfarin?
- Were there multiple strengths of the medication in the medication cart and did the nurse administer an incorrect dose?
- Did the prescribing provider order the strength of the doses administered?
- Did the prescribing provider order INR lab tests?
- Were the tests completed but not reviewed or documented in the medical record?
Blunt End: Investigating the blunt end of the error focuses on the policies, procedures, systems, resources, and constraints surrounding the incident. Here are some blunt end investigation questions for this case:
- What are the policies regarding INR evaluation while on warfarin?
- What tracking systems are in place for patients on anticoagulation medication?
- Is there an adequate process for discontinuing previous medication dosing when new dosing is ordered?
- Are nurses working in this area appropriately oriented to the medication administration process?
- What percentage of the nursing staff are new, float, or agency staff?
- How much overtime or double shifts are nurses in this unit working?
- What communication system is in place for nurses to question medication orders?
Always Look Upstream
When investigating significant errors such as the one above, it is easy to fall into several mental biases.
Attribution error bias: It is easy to pin an error on a character flaw or defect of the clinician at the sharp end of the error. Rather than look for all issues, evaluators stop at the shortcomings of staff members involved in the incident.
Confirmation bias: Making a quick judgment of the cause of an error can lead to accepting evidence that supports that judgment while neglecting evidence that would favor other causes. If an organization is prone to evaluating only the sharp end of a clinical event, evidence supporting this view would encourage investigators to stop looking elsewhere.
Hindsight bias: Actions and outcomes viewed after the fact show an ‘obvious’ path of cause and effect. At the time of the actual event, however, multiple possibilities could have occurred, making the possible outcome less apparent. Investigators must consider the event from a perspective of an unsure outcome (in other words, evaluate the process without “knowing” the error occurred).
By intentionally looking upstream to the blunt end of a clinical situation, the full picture is able to be evaluated and meaningful process and system corrections can be made; leading to reduced risk of future error.
In the case presented above, faulty medication discontinuation practices, poor interdisciplinary communication (both written and verbal), along with inconsistent medication validation at the point of administration contributed to the poor patient outcome.
How do you evaluate clinical error in your setting? Please share your process in the comments section of this post.
Leave a Reply