One in ten doctors and NURSES abuse drugs or alcohol. Is this surprising to you? It was to me when…
Read More

One in ten doctors and NURSES abuse drugs or alcohol. Is this surprising to you? It was to me when…
Read More
Correctional nurses must quickly develop a trust relationship with their patients in order to collect accurate data and effectively evaluate…
Read More
Correctional nurses are often called upon to balance their professional duty with the realities of a secure environment. This can…
Read More
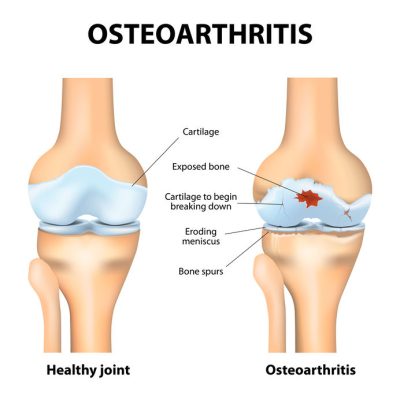
Osteoarthritis and Rheumatoid Arthritis are both debilitating diseases that affect millions of individuals in the United States. In the correctional environment,…
Read More

Arthritis is one of the top five chronic conditions found among our patient population, yet managing this debilitating condition is…
Read More
Correctional nurses pride themselves on objectivity, fairness, and professionalism. Yet like all humans, we carry unconscious assumptions that can influence…
Read More